
So tomorrow is the end for me. I’ve been on my pediatric rotation now for 2 weeks, seen a lot of interesting cases, worked in both an outpatient clinic and an peds emergency room (thank you site for offering that!) but tomorrow I start in the neonatal intensive care unit (NICU) under a (supposedly) intense attending who’s out for medical student blood! So far my medical experience has been fairly… easy? All the undergrad talk of attendings out to destroy their students through aggressive questioning on topics clearly over our heads, going home crying, and hating life… just hasn’t been the case. I’ve worked with wonderful doctors and their incredible staff, all of whom have been more than comfortable when I flat out say “sorry, I have no idea what the answer is“. And for this I’ve been incredibly grateful! This may change tomorrow, but you know what, gotta be PIMPed hard a couple times at least before graduation, right? So I’ve been studying all day on NICU specific topics and I’m here to share what I’ve learned (go me!):
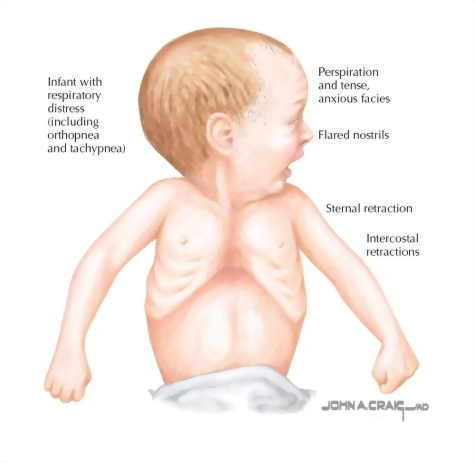
Neonatal Respiratory Distress: very common reason babies end up in the NICU. Transitioning from intrauterine to extrauterine life is incredibly complex and and physiologically demanding on the respiratory system. Here are the 3 most common disorders according to UpToDate:
- Transient Tachypnea of the Newborn (TTN) – Typically “late preterm” infants delivered via c-section at 34-37 weeks old present within 2-hours of delivery. Newborn alveolar fluid fails to clear (presumptively caused by non-active amiloride-sensitive sodium channels (osmotic gradient) & inadequate transepithelial hydrostatic pressure) causing respiratory distress. CXR demonstrates bilateral perihilar linear streaking with engorged lymphatic & blood vessels. Spontaneously resolves in 1-2 days.
- Respiratory Distress Syndrome (RDS) – preterm infants (increased risk in diabetic mothers) present with cyanosis soon after delivery due to inadequate surfactant (desaturated palmitoyl phosphatidylcholine) production. This chemical reduces alveolar surface tension therefore reducing the respiratory effort. CXR demonstrates diffuse, reticulogranular, ground glass appearance with low lung volume. Treatment includes antenatal glucocorticoid, early intubation with surfactant therapy and ventilatory support (CPAP or PEEP).
- Persistent Pulmonary Hypertension (PPHN) – Term infants develop poor pulmonary vascular beds results in elevated pulmonary vascular resistance (PVR) causing a R>L heart shunt and ultimately hypoxemia. Associated with perinatal depression, bacterial infection, poor intrauterine growth, non-reassuring fetal heart rate patterns, tricuspid insufficiency, sepsis, meconium aspiration syndrome and congenital diaphragmatic hernia. CXR variable.
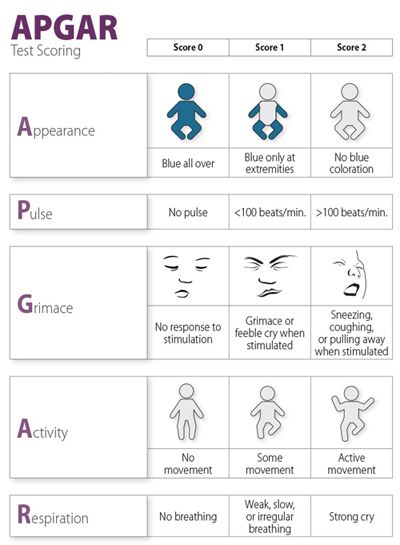
APGAR Score! Obtained 1-minute and 5-minutes following delivery:
Stanford Medicine Newborn Nursery Photo Gallery: Better to see pictures before the real thing! A classmate shared this website with me which includes hundreds of neonatal images curtsey of our pals at Stanford. Thanks guys!
Neonatal Jaundice: A combination of shorter neonatal RBC lifespan, higher RBCs load, slower liver conjugation (and possible metabolic dysfunction) result in supra-physiologic bilirubin levels following birth. While some degree of jaundice is expected and normal, sustained elevated levels force bilirubin across the blood brain barrier and contribute to irreversible neurological damage (kernicterus). Therefore phototherapy (blue light at 420-480nm wavelength) is used to transform non-water soluble trans-bilirubin into water soluble (excretable) cis-bilirubin (lumirubin). While the exact values for when to utilize phototherapy can vary depending on gestational age, hours post delivery, and risk factors, bilirubin >12mg/dL at 24-hours of age for a healthy 38 week baby a starting point. UpToDate
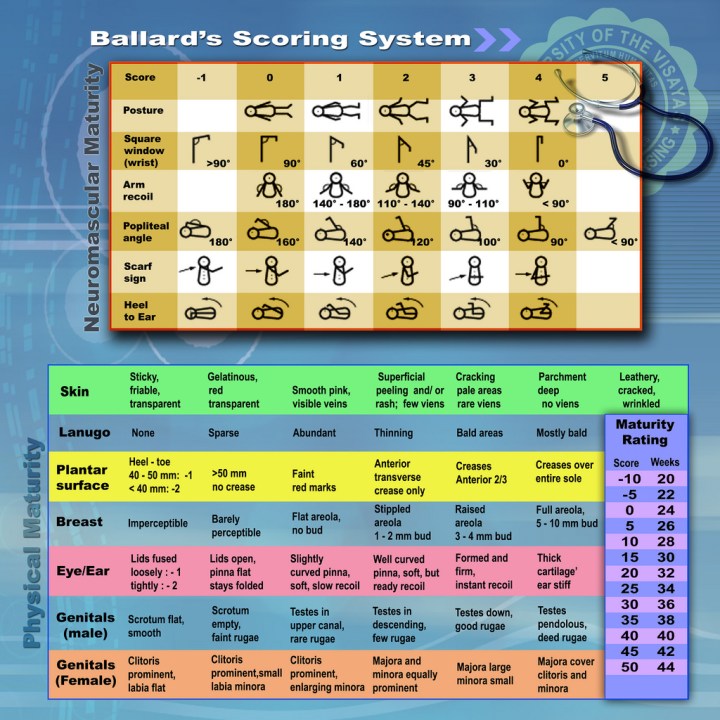
Ballard Score for Determining Gestational Age of a Newborn: This was one I’ve only read about in passing and contains 2 parts: First, the newborn is carefully placed through a series of passive motions where the responses are compared with predetermined angulations/positions (provided below). Second, the child is simply observed, awarding points for each characteristic identified from hair, eyes, breasts, etc. I was only able to locate a excellent, yet archaic, YouTube video demonstrating every criteria which I’ve include below (It’s a 5-part series so you’ll have to watch them all to see everything. Sorry!):
Intrauterine Growth Restriction: Coming Soon!
Delayed Cord Clamping is Beneficial: A recent article by the American College of Obstetrician and Gynecologists (ACOG) found that delaying umbilical cord clamping by 30-60 seconds post-delivery provides numerous newborn benefits. Preterm – improved transitional circulation, better RBC volume, decreased blood transfusions, lower brain hemorrhage AND necrotizing enterocolitis. Term benefits – increased hemoglobin and iron stores for several months, helping prevent iron deficiency during year 1 (which correlates to cognitive, motor, behavioral impairments)

Attendings like that are assholes. Don’t mind him, take what he dishes out, pass shelf and move on. I had a guy who was a dick in Rheumatology, I just focused on the patients, even if you’re only a Med student you can still make a difference by explaining and spending extra time with pt or their fam.
LikeLiked by 2 people