
So I’ve officially been on my Peds service for a full 2-days and I’ve already learned a lot! Kids are fun, parents are great, and the pace is nothing like the emergency room or even occupational health, which I just finished after 3 months. It’s definitely a welcomed change. 🙂 While my immune system is in overdrive attempting to keep me alive just long enough to see the next sick child, I’ve slowly picked up a few little tips & tricks along the way which I thought I would share to potentially help out the next student (awww how nice of me!). I’ll keep updating this list as the weeks progress so sit back and enjoy knowing your just that much more prepared than the next & last rotating student. 😉 Now let’s begin!
- Mothers do not like talking about their child’s weight: Mom’s bring their children in for all sorts of reasons. Most are justified, other times not so much. But what shocked me was the fact that mothers will discuss in great detail literally anything potentially harming their kid’s health, except weight. It’s such a touchy topic! Unfortunately, as a whole, they seem to take any comment on their kid’s plus size as a personal attack on their motherly abilities and it couldn’t be further from the truth. Already I’ve seen numerous moms when they sense the ‘talk’ approaching say “I left my last pediatrician since all he wanted to talk about was my son/daughter’s weight“. The comment is so profound that typically only a casual one-liner follows rather than a thorough discussion/intervention that’s required to actually incite change. But it’s a gamble. Do you forcibly press the topic hoping to safely travers the touchy subject while potentially angering the parent and then losing them in followup, or simply bite the bullet and divert your efforts to literally anything else. Take away: Choose your battles wisely or at least know exactly how you’re going to phrase things since those words may be your last.
- Children are constantly being compared. Whether it’s to themselves in their previous visits or to other kids their age, it’s the only speciality I’ve seen do this. For example obesity for adults is rigidly defined as a BMI between 25-29.9 (height/weight squared) while a child is obese when their BMI is >95% of other children their age. Their head circumference, height and weight are always recorded. Just know this, trending to the medium is ok, staying where they’re been is ok (as long as it isn’t at one extreme or the other), but “falling off the curve” or rising above it is not. Unless it weight. Jk.

- Albuterol is not all good. It is a B2-agonist & it works wonders opening up the airway. However, parents (and I’ll be honest, initially me) assumed everything gets better following a breathing treatment. Not always the case. A lot of child once their airway is patent release a significant amount of trapped mucus and all that gunk wants to come out. Now! The child can go from wheezing to hacking up a lung in a matter of minutes and when you’re not expecting it, it’s a frightening thing. Have the parent informed of this prior to initiating treatment and even suggest the child thump on their chest to help dislodge any trapped mucus to help expedite the process. Yay for phlegm!
- Everything is viral unless strongly proven otherwise. While dishing out antibiotics like candy 20 years ago might have been all the rage (no citations) it’s very much taboo now. Unfortunately, no matter how much it’s stressed, many patients do not complete their prescribed antibiotics to their entirety and that’s a very bad thing. While killing off 99% of the bug might result in your child initially feeling better, stopping the antibiotic prematurely results in that hardened 1% surviving and then multiplying (now completely resistant to the first antibiotic) and ultimately the patient’s cold returning with a vengeance. Furthermore, remember that all medications cause side effects. Let me repeat this for it’s extreme importance, ALL MEDICATIONS HAVE SIDE EFFECTS. Even Tylenol & Aspirin cause problems. So pediatricians have rightfully developed laser vision to detect any reason to NOT prescribe an antibiotic but instead carefully select which patients can safely “wait it out” and let the disease get better on its own, and that’s a wondrous thing. So when presenting, you better have a slam dump reason for suggesting an antibiotic or you’re going to get the look. Just saying.
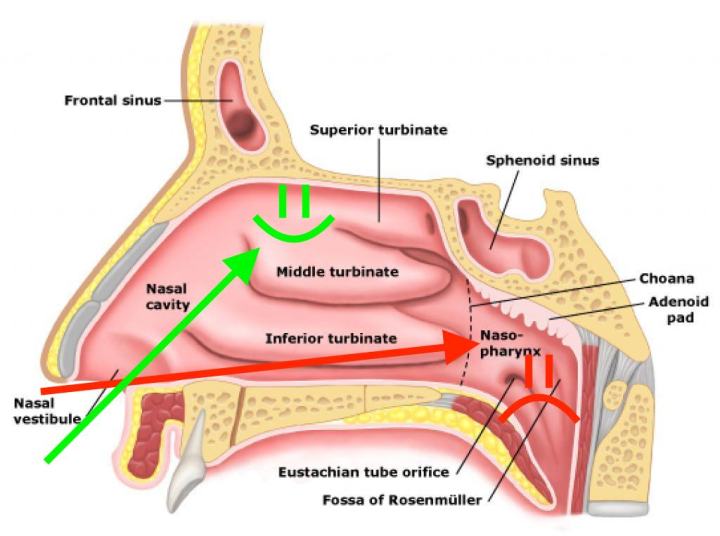
- Direct nasal spray with purpose. If the child’s nose is plugged up and you’re prescribing a spray, have the patient direct it into the outside walls of the nostrils rather than straight back. But directing back is logical, right? Wrong. Doing so dispenses the chemical past its intended target on instead all over the back of the throat which is NOT where the congestion is. The anatomy of the nose is such that the turbinates (which are the structures that swell and block air flow) are immediately inside the nose and pushing the applicator past them completely defeats their purpose, especially when the majority of chemical’s work by shrinking them. Just use anatomy & common sense, right?
- Don’t give kids a choice, make it for them. To end on a funny note, today I thought I would be nice and offer the choice of 2-cool stickers to a child in the hopes he’d be able to choose better than me and be happier. I couldn’t have been more wrong. I showed him two, he picked one, I retracted the other, he panicked. I reintroduced mine, which he delightfully exchanged for his, and then he proceeded to cry excessively. His mother said it was ok and I left. All I heard for the next 5-minutes from outside in the hall was how he wanted the other one. Haha. I of course cracked and gave him mine (or did I) learning a valuable lesson: it’s all of nothing with the little ones. 😉

Hope this was helpful and fun! Enjoy
