
So this is critical. When your clinic gets crazy busy and your preceptor leans over and says “write out a prescription for… ” you better not have a deer in the headlights look (like I’m sure I did the first couple times). Granted, while there is a universal system in place for writing out prescriptions via old school pen & script pad, most major hospitals have upgraded to electronic prescriptions. However, if you’re going to work in a family medicine clinic, older private practice and especially psychiatry, welcome back to the stone ages. So here’s my quick guide to drafting your first script like a champ and not being one of “those” meds students.
First, make it your mission upon entering a new practice to study a completed prescription. Everything from formatting to most critically, location of the pad itself! Sounds obvious right? Wrong. When the clinic gets busy and your preceptor asks you to be his scribe, if you don’t even know where the script pad is, game over. You’ve lost your chance to be helpful and the job’s immediately been given to someone else. Don’t let that happen. Furthermore, when the attending drafts up a new prescription don’t let yourself be passive and your brain go to sleep. I know mine does. Predict what he’s going to write next and be mindful as to where everything is going, line-by-line. Format is key. One incorrectly placed word/number and that paper will be ripped from your hands and shredded before you even know what happened.
Here’s what a basic script should look like:
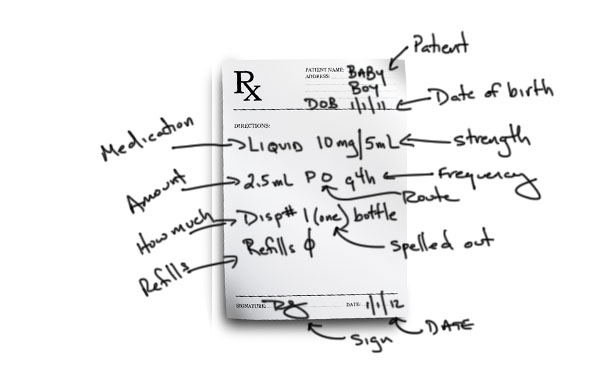
Now let’s go line by line to make you the prescription writing machine!
- Top: Patient’s full name & D.O.B.
- Line 1:
- Medication name. THIS MUST BE SPELLED CORRECTLY. If I’m even 1% uncertain I simply bust out my phone, drop the name in google, make sure it’s perfect and move right alone.
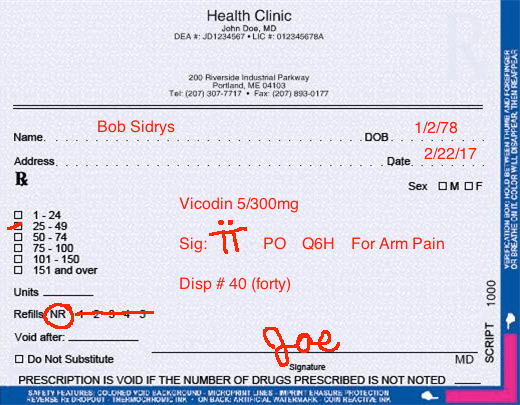
- Strength. Some drugs have 2 active components (like listed above). Ex: Vicodin is a combination of hydrocodone and acetaminophen, starting at 5mg & 300mg which increase. My prescription would read “Vicodin 5/300mg“.
- Line 2:
- How many pills should be taken at one time. This is written interestingly. The world of pharmacology is a combination of traditional Latin and unique tricks to eliminate potential errors. First, start with the word “Sig“. This is Latin for signetur, basically means you’re instructions to the patient. Next, you will use something similar to roman numerals with corresponding dots. Take one pill? Capital “T” with one dot overhead. Take 2? Capital “T” but with 2 vertical bars with 2 dots, ect.
- Via which route. “PO” is Latin again for “by mouth”.
- How often. Two basic options here: “PRN” simply means “as needed”, while “Q” stands for every & “H” stands for hours. So you want your patient to take the medication every 6 hours, write “Q6H”.
- Reason for the prescription. You’ve seen your grandmother’s medicine cabinet, right? There’s a million drugs in there. You want your patient to be able to refer back to a medication at any time and know exactly why she got it and take it for that reason only. Ex: Sig: T (dot) PO Q6H for arm pain.
- Line 3:
- How many pills should they receive. It’s simple math time! Basically, you want your patient covered for a predetermined number of days in the event they take the medication exactly as prescribed. Want their pain covered for 5 days? Well if they’re popping 2 pill every 6 hours, with 24 hours in a day, they’ll need 40 pills. This is written as “Disp. #“, followed by the number. Simple. Importantly, you must additionally Spell out the number dispensed so no alterations can be made. Say you write down “20” but your maniacal patient adds a zero? Now you’ve technically ordered 200 tablets and you as the prescriber is in big doo-doo. Thank you “pharmacy gods” for being smart. Two side notes: Some docs move quickly and have no time for math. They’ll write “QS” and move right along. It stands for “quantity sufficient”, meaning they want the pharmacist to determine how many pills the patient needs via their above instructions. Personally, I like doing the math myself but that may change after writing my 1,000th prescription. Second: sometimes there is a checkbox on the side estimating an average of how many pills to dispense. Select the appropriate box and cross out the other options ON BOTH SIDES, again, eliminating any potential alterations. Ex: Disp. # 40 (forty).
- Line 4:
- Refills. If there’s a pre-provided list of numbers simply check yours and cross out the others.
- Bottom: Your attending’s scribbly signature and today’s date.
Here’s my example:
A couple interesting points I’ve picked up along the way:
- There is no such thing as narcotic refills. You need a refill? You must come in and be reexamined by a physician and a new prescription is written. HOWEVER, there is one way around this I’ve seen physicians do: future date your prescription. Have the order filled 30 days after todays visit. That way the patient can’t fill it now and their current order will be consumed by then. Not sure how I feel about this one.
- Only give your patient one variability. Never say “take 1-2 pills every 4-6 hours”. They could take that, AS PRESCRIBED, anywhere from 1 pill every 6 hours to 2 every 4. Huge difference!
Hope this helps. If you want to go bug-wild with abbreviations feel free to check out this website. Enjoy!
Editor: MDL
