
So today my preceptor gave us 2 cases! This was a complete surprise since (1) we’ve never done more than 1 case in a day and (2) it’s a Monday, our busiest day of the week. Thankfully not today. I was especially excited for the first case since its topic was “GI Bleed”. Instead of presenting the whole case, for now I’m just going to explain the mnemonic for remembering the causes for 99% of the gastrointestinal bleeds you see in the emergency room. U.V.A.MED – NADIR.
- Ulcer: Peptic (stomach) & duodenal (intestinal). Diagnostic clues would be pain exacerbated by eating (peptic ulcer since you’re stomach is going to increase acid production (H+) which will further damage the sensitive ulcerous tissue) or relieved by eating (duodenal ulcer since the duodena produces bicarb (HCO3-) which temporarily neutralizes acidic contents). Either can perforate leading to free air under the diaphragm and a septic patient. Do not take these lightly.

- Varices: Superficial esophageal veins can dilate due to increased pressure from a congested/diseased liver and bleed. This can be anywhere from almost undetectable except via guaiac stool test to a life threatening rupture where the patient will vomit a swimming pool worth of blood and exsanguinate them to death in minutes.

- Arteriovenous Malformation: The unwanted union of an artery to a vein. Patients can be born with these or develop them due to some disease process.
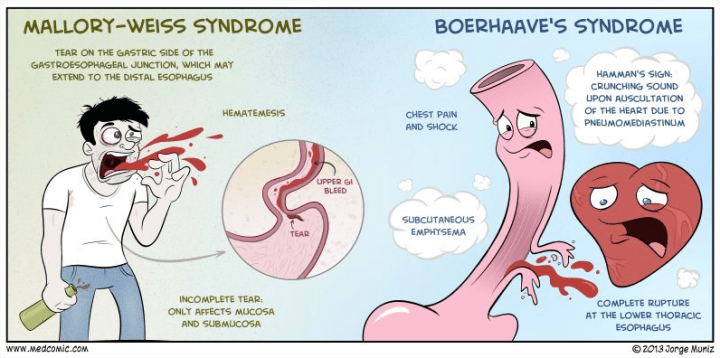
- Mallory Weiss/Boerhaave’s: These 2 distinct tears in esophagus are caused by excessive vomiting. Mallory Weiss is typically seem with your “weekend warriors” who party too hardy, then vomit repeatedly, producing a transverse tear in their esophagus that bleeds. While not a fun bleed, Boerhaave’s is significantly worse. With this type, a bulimic person (vomits after eating) retches repeatedly producing a full thickness tear of the esophagus resulting in gastric contents in your chest cavity, significantly worse bleeding and eventual sepsis. These are the patients that crash hard and fast!
- Esophagitis/Gastritis/Duodenitis: The suffix -itis simply means inflammation. If any part of the upper GI track is inflamed, it’s irritated and caustic gastric contents can damage it enough to bleed.
- Dieulafoy’s Lesion: Never even heard of this one before. My preceptor even offered us $1,000 if we already knew the name. It’s a specific AVM in the fundus of the stomach which has a propensity to bleed.
>LIGAMENT OF TREITZ< tissue in the small intestines which divides the upper from lower GI tract
- Neoplasm: Cancerous cells produce enzymes which digest cellular material around themselves. In doing so, they eventually rupture blood vessels in their conquest to grow. This is why not only colonoscopies are recommended to adults >50 every 5 years, but alternatively yearly guaiac tests since bloody poops can mean cancer too.
- Arteriovenous Malformation: as stated above.
- Diverticulosis/Diverticulitis: Diverticulosis is when an intestinal outpouching develops due to simultaneous elevated bowel pressures on a weak wall. Studies suggest 50% of people age 50 have at least one with your chances of developing one increase by 10% every decade. While these pouches never return to normal they are medically insignificant. However problems arise when food particles get trapped inside them and wall themselves off resulting in bacterial overgrowth and infection, eventually turning into diverticulitis. These frequently bleed.

- Ischemia/Infection: Ischemia, or the lack of oxygen, is commonly caused by a clot elsewhere in the body lodging itself in the intestinal arteries, starving the region enough to starve, die and eventually bleed. Clinically you would see pain that appears out of portion to the story. Infectious causes of bloody stool are Salmonella, Shigella, Hemorrhagic E. Coli, and Campylobacter. (all to hopefully be covered in greater detail later)
- Roids. External & Internal Hemorrhoids.
I hope this fairly comprehensive list of GI bleeds helps at least one soul out there. So far we have UVAMED-NADIR or… ulcer, varices, AVM, Mallory Weiss/Boerhaave’s, esophagitis/gastritis/duodenitis, Dieulafoy’s Lesion, neoplasm, AVM, diverticulosis/itis, ischemia/infectious and roids.
Reviewer: MDL
